![]()
What Organizations Need To Know About Aging In Adults With
Part of the Essentials of Dementia Capable Care Series
Jeff Owens - contact[AT]autism-101.com
This presentation uses “Identity-First” language to refer to others with .
Presentation available at: https://slides.autism-101.com
Who Are You?
- I’m Jeff Owens
- I’m a late diagnosed autistic person
I grew up feeling like an alien, inhabiting the wrong planet.

Which is why Mr. Spock became my favorite TV character.

Spock likes cats.

And I like cats. (Ginger & Jet)

Spock likes chess.

And I like chess.

Spock likes computers, and so do I.

Spock likes music.

And so do I.

Spock has trouble understanding his emotions, and so do I.

Last year I received the “Live Long and Prosper” award from the Nimoy-Knight Foundation.

Which was a great honour for me. Past recipients include Dr. Temple Grandin, Billie Jean King, and Whoopie Goldberg.

I drink coffee from my Star Trek mug every day.

And I use a Star Trek mousepad.

I like detective shows.


I love music composed by John Williams.

I run the Autism-101.com website.

As well as AutismInTheMedia.com.

What Is ?
- is a neurological and developmental difference
- It is naturally occurring
- It is not a disease 😷
- It can’t be cured
- It has always existed
Autistic People Differ
“If you have met one autistic person
you have met one autistic person.” [1]
— Dr. Stephen Shore ( advocate)

Why Is This Important Now?
The Timeline of Invisibility
Why didn’t they get diagnosed 40 years ago?

- 1943-1944: Kanner & Asperger define the condition (mostly in children).
- 1980 (DSM-III): “Infantile ” enters the DSM. Strict criteria.
- 1994 (DSM-IV): Asperger’s Syndrome added. The beginning of broader recognition.
- 2013 (DSM-5): ASD becomes a spectrum; allows for adult diagnosis more easily.
“We aren’t part of an epidemic.
We are part of an awakening.”
— Autism-101
ASD Support Levels
- Level 1 - requires support
- Level 2 - requires substantial support
- Level 3 - requires very substantial support
First Person Diagnosed in U.S.
Donald Triplett - was diagnosed by Leo Kanner in 1943

Donald Triplett
- Born: Forest, Mississippi in 1933.
- College: he graduated with a bachelor’s degree in mathematics and French.
- American Banker: he worked for 65 years at a local bank.
- Music: he had perfect pitch.
- Savant: he could do rapid mental multiplication.
- Book: featured in the book, In a Different Key, later adopted into a documentary.
Who Are “Older Autistic Adults”?
Today, we are focusing on those 50+, but specifically two groups:
- Diagnosed early: now aging.
- “Lost Generation”: diagnosed late in life, or still undiagnosed.
Why Were They Missed?
- Diagnostic criteria historically focused on young, white males with high support needs.[6]
- Masking or Camouflaging to survive education and employment.
Traits attributed to other things: “quirky,” “shy,” “difficult,” or misdiagnosed with personality disorders/anxiety.
What Triggers a Late Diagnosis?
Often, a life event drastically alters the person’s capacity to cope:
- Burnout: Decades of masking finally depletes energy reserves.
- Hormonal Shifts: Perimenopause and menopause can intensify sensory/executive function struggles.
- Major Transitions: Retirement, becoming an empty nester, or loss of a spouse removes stabilizing routines.
- The “Genetic Mirror”: Seeing their own traits while their child or grandchild is being assessed.
The Diagnostic Journey
As detailed in books like Lost & Now Found [7] , diagnosis is complex:
Relief & Validation
"I'm not broken; I'm Autistic. There is a name for this."
Grief & Anger
Mourning lost opportunities and decades of struggle without support.
Re-evaluation
Reviewing one's entire life history through a new lens.
Case Study: “Susan” (Age 64)
- Background: Retired librarian. Always called “shy” and “rigid.”
- The Trigger: Husband passed away 2 years ago. The loss of his support (handling bills, driving, social buffer) caused a collapse.
- The Misdiagnosis: Diagnosed with Treatment-Resistant Depression and Early Onset Dementia due to “confusion” (which was actually brain fog and burnout).
- The Realization: Read a memoir by an autistic woman and recognized herself.
and Intellectual Disability (IDD)
- Overlap: A significant portion of autistic adults also have a diagnosis of Intellectual Disability (30-40%).[8]
- Complexity: Aging impacts functional skills differently when neurodivergence and IDD co-occur.[9]
- Support Needs: High support needs may shift from educational/vocational to clinical and residential as the person ages.[10]
The DS-ASD Profile
- Down Syndrome and (DS-ASD) Individuals with Down Syndrome have a significantly higher prevalence of than the general population.[11]
- Unique Presentation: Social-communication challenges may be more pronounced than in peers with Down Syndrome alone.[12]
- Organizational Insight: Care protocols must be tailored to both the genetic profile and the autistic sensory profile.[13]
APP Gene On Chromosome 21
Location of the APP gene on chromosome 21 in humans

Alzheimer’s and Dementia Risks
- Heightened Risk: Autistic adults with IDD have nearly 3 times the risk of early-onset Alzheimer’s compared to non-autistic peers.[14]
- Down Syndrome Link: Due to the APP gene on chromosome 21, nearly all adults with Down Syndrome exhibit Alzheimer’s pathology by age 40.[15]
- Diagnostic Overshadowing: New dementia symptoms are often wrongly attributed to “just their ” or “typical IDD behavior”.[16]
Co-occuring Conditions
- Will likely have other issues
- Ex. ADHD may occur in 40% or more of autistic people [17]

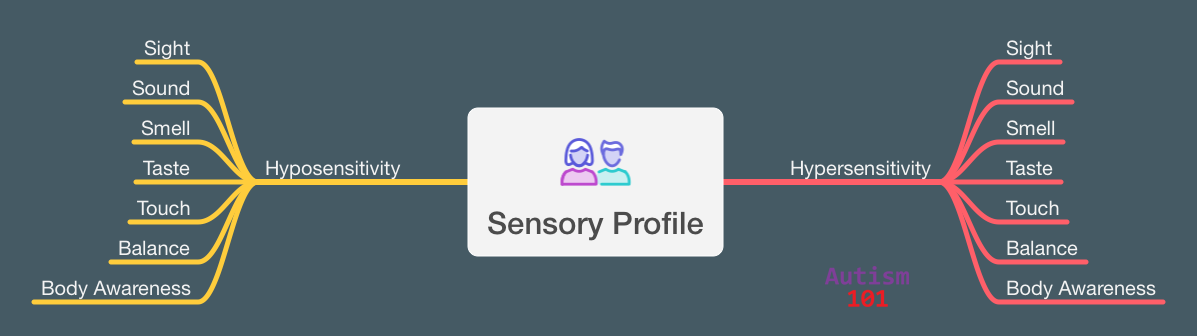
Sensory Differences
“Processing everyday sensory information can be difficult for autistic people. Any of their senses may be over- or under-sensitive, or both, at different times.” [18]
— NAS
Sensory Profiles
- Unique to individual
- Hyposensitive, hypersensitive, or both
- Can change day to day
- Are well outside the normal ranges
- Impacts what we like to do
Do Sensory Issues “Mellow” With Age?
Short Answer: No. They often become harder to manage.
- Older autistic adults report lower ability to “cope” with sensory input. The energy used to “mask” or “push through” in their 30s is gone.[19]
- Age-related hearing/vision loss increases cognitive load. The brain works harder to interpret data, leading to faster overload.[19]
- After age 40, the autistic nervous system may regulate stress less efficiently, making sensory triggers feel more physically painful.[19]
The “Double Whammy”
Aging and interact bidirectionally:
Diagnostic Overshadowing
- The Barrier: Clinicians may ignore new health issues (like pain or cognitive decline) because they focus only on the developmental disability.[21]
- Communication: Non-speaking or minimally-verbal adults may express pain or dementia-related confusion through “challenging behaviors”.[22]
- Organizational Task: Staff must be trained to look for changes in baseline behavior as medical indicators.
Healthcare Barriers
- Communication Mismatches: Difficulty describing pain accurately; doctors misinterpreting flat affect or direct/blunt communication as non-compliance.[23]
- Sensory Overload in Clinics: Bright lights, waiting rooms, and physical exams can lead to care avoidance.
- Co-occurring Conditions: Higher rates of anxiety, depression, GI issues, and sleep disorders often complicate geriatric care.[24]
Sensory and Cognitive Shifts
- Sensory: Natural age-related hearing/vision loss combined with autistic sensory processing differences can be overwhelming and disorienting.
- Executive Function: Aging impacts working memory and processing speed. For an autistic brain already working hard to organize, this can lead to significant functional decline quickly.
- Burnout Recovery: Bouncing back from sensory or social overload takes significantly longer at 60 than at 30.
Shrinking Support Networks
- Loss of “Buffers”: Many older autistics relied heavily on parents or a spouse to navigate the social world. Losing them is catastrophic.
- The “Group Home” Fear: Intense fear of losing independence and ending up in communal senior living, which is rarely sensory-friendly.
- Financial Vulnerability: Due to lifetime underemployment (common in the lost generation), financial resources for aging may be scarce.
“Autistic Advantages” in Aging
Many older autistic adults possess unique resilience factors:
- Solitude as Strength: Often better equipped to handle alone time than neurotypical peers.
- Passionate Interests: “Special Interests” provide deep engagement, cognitive protection, and joy.
- Non-Conformity: Less pressure to keep up with societal expectations of “how to act”” at 50+“.
Organizational Supports: Sensory Audits
- Evaluating the Environment: for Dementia-Capable Care.
- Visual: Reduce flickering fluorescent lights and high-contrast patterns that cause disorientation.
- Auditory: Identify and mitigate “background” hums (HVAC, machines) that increase cognitive load.
- Tactile: Ensure clothing and bedding textures remain consistent to prevent sensory-driven distress.
Communication Protocols
- Direct and Literal: Avoid metaphors or vague instructions; autistic people with dementia need “processing time”.
- Visual Aids: Use schedules and pictures to reduce the load on working memory.
- Stabilization: Routine is a clinical tool. Predictable environments reduce the anxiety associated with cognitive decline.
Moving Forward: Neuro-Affirming Care
- Preserving Energy: Unmasking and sensory aids (headphones, stimming) are energy-conservation tools for seniors.
- “Nothing About Us Without Us”: Even those with advanced dementia or IDD should have their preferences and sensory comfort prioritized.

References 1 / 5
References 2 / 5
References 3 / 5
References 4 / 5
References 5 / 5
Check Your Knowledge
Question 1
True or False:
The “Double Whammy” refers to the bidirectional interaction where age-related cognitive slowing can intensify lifelong autistic traits like sensory sensitivity.
TRUE
Question 2
True or False:
Autistic adults with Down syndrome (DS-ASD) may follow a different aging trajectory, including a higher risk for early-onset Alzheimer’s disease.
TRUE
Question 3
True or False:
“Diagnostic overshadowing” occurs when a clinician mistakenly attributes new dementia symptoms to a person’s pre-existing autism or IDD.
TRUE
Question 4
True or False:
Sensory issues in autistic adults usually resolve by age 65, making sensory-friendly environments less critical in senior care settings.
FALSE
Sensory processing issues often persist or intensify with age.
Question 5
True or False:
Because of communication mismatches, an autistic person may express physical pain or dementia-related distress through “behaviors” rather than verbal reports.
TRUE
Question 6
Multiple Choice:
Which organizational support is most effective for reducing “burnout” in aging autistic adults with IDD?
- A) Increasing the number of mandatory group social activities.
- B) Performing “sensory audits” of living spaces to reduce lighting and noise triggers.
- C) Requiring the person to “mask” their traits to fit into a standard nursing home.
- D) Limiting access to “special interests” to encourage broader social interaction.
CORRECT ANSWER: B
Question 7
Multiple Choice:
In the “Lost Generation” of autistic seniors (aged 50+), a common trigger for a late-life functional collapse is:
- A) The loss of a primary “social buffer” or caregiver, such as a parent or spouse.
- B) A sudden interest in new, high-energy hobbies.
- C) Moving to a more crowded, urban environment.
- D) Reaching the age of official retirement.
CORRECT ANSWER: A
Question 8
Multiple Choice:
For organizations supporting adults with both and Alzheimer’s, clear communication should prioritize:
- A) Abstract metaphors to explain medical procedures.
- B) Literal, direct language with extra time allowed for cognitive processing.
- C) Rapid-fire instructions to keep the person engaged.
- D) Relying solely on non-verbal cues.
CORRECT ANSWER: B
Question 9
Multiple Choice:
Why is “Unmasking” considered a healthy aging strategy for autistic adults?
- A) It helps them blend in better with neurotypical peers.
- B) It helps them develop more “typical” social skills.
- C) It preserves limited energy reserves by stopping the exhausting performance of “neurotypicality.”
- D) It is only useful for children, not seniors.
CORRECT ANSWER: C
Question 10
Multiple Choice:
A “Neurodiversity-Affirming” approach to geriatric care for those with IDD means:
- A) Focusing entirely on “curing” autistic behaviors.
- B) Validating the individual’s lived experience and identity without demanding a “cure.”
- C) Only providing support to those with a formal childhood diagnosis.
- D) Designing programs that treat all seniors exactly the same regardless of neurology.
CORRECT ANSWER: B